
Shoulder Injuries Part 1 - Five Joints to Consider Not Just One
- Dr. Brian Abelson DC
- Apr 11, 2023
- 8 min read
Updated: Jun 14, 2024

In this four-part series on shoulder complexities, we'll delve into the shoulder's intricate design, embracing its five joint structures, the pivotal role of the rotator cuff, the diagnostic challenges it presents, and the impressive seventeen muscles that connect to it. We aim to offer a holistic view, highlighting manual therapy and exercise treatment recommendations. The shoulder's design ensures a balance between mobility and stability. When this balance is disrupted, susceptibility to injuries heightens."
Article Index:
Introduction
5 Joints
Conclusion & References
Introduction
The shoulder complex is an intricate and sophisticated anatomical system that comprises the glenohumeral joint and four other osseous components, muscular attachments, tendinous insertions, ligamentous support, fascial elements, and neurovascular constituents.
The scapula, a key component in this assembly, boasts connections to an astounding seventeen distinct muscular structures. In concert, the skeletal, muscular, and soft tissue elements of the shoulder work synergistically to establish a delicate equilibrium of forces, ensuring both mobility and stability. However, when this finely tuned homeostasis is perturbed, the shoulder becomes increasingly predisposed to injuries and functional impairments.

Understanding the Unique Nature of Your Shoulders
Our shoulders are ingeniously designed to offer a remarkable range of motion, albeit at the expense of stability. The shoulder girdle is relatively unstable compared to other joints in the body. This inherent instability can immediately affect other anatomical structures when shoulder injuries occur.
To effectively address a shoulder injury, it is crucial to comprehend the interconnections, relative movements, and kinetic chain associations among the shoulder's various soft-tissue and skeletal structures. To begin, let's explore the shoulder joints.
It's important to note that we have a wealth of information to share on this complex subject. In this initial segment, we'll focus on the shoulder joints. Subsequent articles in this series will explore other affected structures, diagnostic approaches, and potential solutions. So, stay tuned, or feel free to jump ahead to the section that sparks your curiosity!

Anatomy and Biomechanics of Shoulder Joints
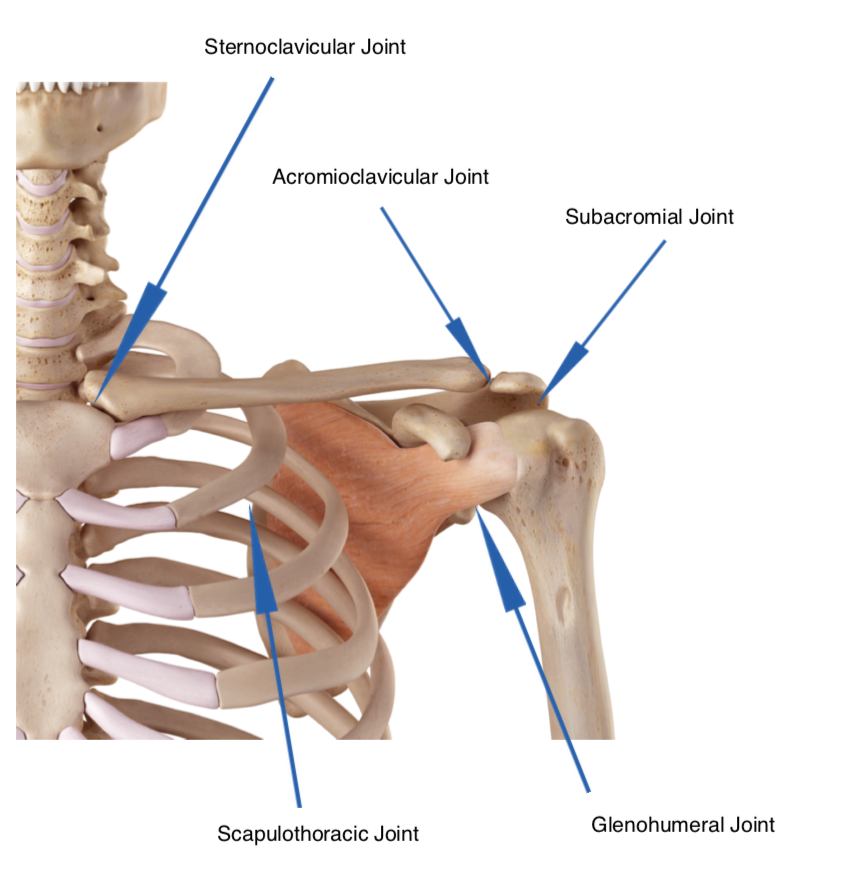
Contrary to popular belief, the shoulder is not composed of just one joint. Instead, it encompasses five distinct joints that work together to facilitate movement.
The shoulder girdle comprises five crucial joints, including three traditional joints and two physiological joints:
Glenohumeral Joint.
Acromioclavicular Joint.
Sternoclavicular Joint.
Scapulothoracic Joint (physiological joint).
Subacromial Joint (physiological joint).
Appreciating the interconnections among the components of these five joints is crucial for effectively addressing shoulder injuries.
Remember that joints do not function independently; a limitation or dysfunction in one region invariably leads to compensatory adjustments elsewhere in the body. Addressing these compensatory mechanisms along the joint's kinetic chain is often necessary to fully resolve a shoulder injury.

Glenohumeral (GH) Joint
The glenohumeral joint, also known as the shoulder joint, is a ball-and-socket joint filled with synovial fluid. This fluid reduces friction between the articular cartilage during movement in synovial joints. The glenohumeral joint facilitates flexion, extension, adduction, abduction, and arm internal and external rotation.
Glenohumeral Instability
During shoulder joint examinations and translation tests, practitioners frequently encounter glenohumeral instability. Studies indicate that prolonged periods of shoulder instability, specifically glenohumeral instability, can initiate a cycle of micro-trauma. This, in turn, may lead to secondary impingement syndromes that often result in persistent shoulder pain.
Anterior shoulder instability, characterized by laxity of the anterior capsule, is often associated with issues in the posterior shoulder capsule, significantly impacting the shoulder's kinetic chain.

When the posterior shoulder capsule tightens, it influences the Inferior Glenohumeral Ligament (IGHL) function. The IGHL maintains the shoulder's position within the joint, acting as a supportive hammock or sling for the humerus (humeral head). If the IGHL is not functioning properly, the arm's position shifts, potentially leading to a range of impingement issues (1, 2).

The glenohumeral joint showcases intriguing fascial connections. For instance, the subscapular fascia is continuous with the rhomboid fascia, which subsequently inserts into the glenohumeral joint. Any constraints or forces produced along this fascial line have the potential to impact the functionality of the glenohumeral joint (1).

Acromioclavicular (AC) Joint
The acromioclavicular (AC) joint is situated between the scapula's acromion process and the clavicle's lateral end. The AC joint is classified as a 'gliding' or 'plane type' synovial joint.
The scapula's acromion rotates on the clavicle's acromial end. Although the AC joint is a gliding joint, it functions as a pivot point to enhance scapular motion, which subsequently increases arm rotation. The AC joint's motion is often described as scapular movement relative to the clavicle.
The AC joint is highly susceptible to trauma and degenerative changes (3).

Sternoclavicular (SC) Joint
The sternoclavicular joint is situated between the manubrium of the sternum and the first costal cartilage.
The SC joint represents the sole attachment point of the upper limb to the axial skeleton. This joint enables clavicle movement across three planes, most of which occur in the anteroposterior and vertical planes.

Instabilities due to injuries and osteoarthritic changes are the most prevalent issues associated with the SC joint. The sternoclavicular joint is classified as a saddle-type synovial joint.

Scapulothoracic (Scapulocostal) Joint
The scapulothoracic joint is a 'physiological joint,' which is musculo-tendinous. It forms through articulating the anterior scapula and the posterior thoracic rib cage. The trapezius, rhomboids, and serratus anterior muscles primarily constitute the scapulothoracic joint.
The scapulothoracic joint facilitates gliding movements such as elevation, depression, retraction, protraction, and superior and inferior rotation of the scapula. The joint's movement generally results from a combination of SC and AC joint motion. The scapulothoracic joint enhances arm elevation while offering a stable foundation for the controlled motions between the humeral head and glenoid fossa (4).
The most frequently encountered issues with the scapulothoracic joint are due to abnormal motion patterns. Abnormal shoulder blade motion patterns (scapular dyskinesis) can lead to significant dysfunction. We will explore this topic in part two of "Shoulder Injuries."

Subacromial (Suprahumeral) Joint
The subacromial joint is a 'physiological joint' formed by the articulation of the coracoacromial ligament and the humerus head.
This joint arises from the space between the humerus and the acromion process of the scapula. The subacromial bursa and the supraspinatus tendon primarily occupy the subacromial joint.
Subacromial Impingement Syndrome (SIS) manifests as anterior-lateral shoulder pain during arm elevation. This syndrome is characterized by symptomatic irritation of the subacromial structures, situated between the coracoacromial arch and the humeral head, during the arm's elevation.

Anatomy of the Shoulder
Interested in delving deeper into shoulder joint anatomy and biomechanics?
Take a look at our shoulder anatomy video. This presentation discusses the bones (osseous structures) that comprise the shoulder girdle.
Conclusion
In conclusion, the shoulder girdle has five joints and is a complex and sophisticated structure crucial for our daily activities. Dysfunctions within any of these joints can result in compensations and abnormal motion throughout the shoulder complex. Understanding the interrelationships and biomechanics of these joints is essential for effectively addressing shoulder injuries and dysfunction.
As we proceed to Part 2 of "Shoulder Injuries," we will explore the soft tissue structures connected directly to the shoulder blades (scapulae) and examine how restrictions in any of these structures can easily cascade, leading to the development of abnormal motion patterns (dyskinesis), impingement syndromes, and various other issues. By increasing our knowledge of the shoulder's anatomy and the implications of dysfunction, we can better identify potential problems, prevent injuries, and facilitate rehabilitation when needed.
References - Part 1
Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology: Part I: pathoa-natomy and biomechanics. Arthroscopy 2003;19:404-420
Shuenke, Micheal (2010). Thieme Atlas of Anatomy: General Anatomy and Musculoskeletal System. New York: Everbest Printing Ltd. ISBN 978-1-60406-286-1.
Levangie PK, Norkin CC. Joint Structure and Function : A Comprehensive Analysis. 4th ed. India: JAYPEE; 2006.
Levangie, P.K. and Norkin, C.C. (2005). Joint structure and function: A comprehensive analysis (4th ed.). Philadelphia: The F.A. Davis Company.
Stecco, Carla; Stecco, Carla. Functional Atlas of the Human Fasical System. Elsevier Health Sciences.
Abelson, B., Abelson, K., & Mylonas, E. (2018, February). A Practitioner's Guide to Motion Specific Release, Functional, Successful, Easy to Implement Techniques for Musculoskeletal Injuries (1st edition). Rowan Tree Books.
Magee, D.J. (2014). Orthopedic Physical Assessment. St. Louis, MO: Elsevier.
Palastanga, N., Field, D., & Soames, R. (2012). Anatomy and Human Movement: Structure and Function. Edinburgh: Elsevier.
Wilk, K.E., Reinold, M.M., & Andrews, J.R. (2009). The Athlete's Shoulder. Philadelphia, PA: Churchill Livingstone/Elsevier.
Ludewig, P.M., & Braman, J.P. (2011). Shoulder impingement: Biomechanical considerations in rehabilitation. Manual Therapy, 16(1), 33-39.
Lewis, J.S. (2011). Rotator cuff tendinopathy: A model for the continuum of pathology and related management. British Journal of Sports Medicine, 45(13), 918-923.
Ellenbecker, T.S., & Cools, A. (2010). Rehabilitation of shoulder impingement syndrome and rotator cuff injuries: An evidence-based review. British Journal of Sports Medicine, 44(5), 319-327.
Disclaimer:
The content on the MSR website, including articles and embedded videos, serves educational and informational purposes only. It is not a substitute for professional medical advice; only certified MSR practitioners should practice these techniques. By accessing this content, you assume full responsibility for your use of the information, acknowledging that the authors and contributors are not liable for any damages or claims that may arise.
This website does not establish a physician-patient relationship. If you have a medical concern, consult an appropriately licensed healthcare provider. Users under the age of 18 are not permitted to use the site. The MSR website may also feature links to third-party sites; however, we bear no responsibility for the content or practices of these external websites.
By using the MSR website, you agree to indemnify and hold the authors and contributors harmless from any claims, including legal fees, arising from your use of the site or violating these terms. This disclaimer constitutes part of the understanding between you and the website's authors regarding the use of the MSR website. For more information, read the full disclaimer and policies in this website.
DR. BRIAN ABELSON DC. - The Author

Dr. Abelson is dedicated to using evidence-based practices to improve musculoskeletal health. At Kinetic Health in Calgary, Alberta, he combines the latest research with a compassionate, patient-focused approach. As the creator of the Motion Specific Release (MSR) Treatment Systems, he aims to educate and share techniques to benefit the broader healthcare community. His work continually emphasizes patient-centred care and advancing treatment methods.

Join Us at Motion Specific Release
Enroll in our courses to master innovative soft-tissue and osseous techniques that seamlessly fit into your current clinical practice, providing your patients with substantial relief from pain and a renewed sense of functionality. Our curriculum masterfully integrates rigorous medical science with creative therapeutic paradigms, comprehensively understanding musculoskeletal diagnosis and treatment protocols.
Join MSR Pro and start tapping into the power of Motion Specific Release. Have access to:
Protocols: Over 250 clinical procedures with detailed video productions.
Examination Procedures: Over 70 orthopedic and neurological assessment videos and downloadable PDF examination forms for use in your clinical practice are coming soon.
Exercises: You can prescribe hundreds of Functional Exercises Videos to your patients through our downloadable prescription pads.
Article Library: Our Article Index Library with over 45+ of the most common MSK conditions we all see in clinical practice. This is a great opportunity to educate your patients on our processes. Each article covers basic condition information, diagnostic procedures, treatment methodologies, timelines, and exercise recommendations. All of this is in an easy-to-prescribe PDF format you can directly send to your patients.
Discounts: MSR Pro yearly memberships entitle you to a significant discount on our online and live courses.
Integrating MSR into your practice can significantly enhance your clinical practice. The benefits we mentioned are only a few reasons for joining our MSR team.



Comments